There’s been a bit of a kerfuffle lately, about a new Florida law that prevents pediatricians from asking parents about guns in the home.
There’s one customary question, though, that I’m no longer allowed to ask. In June, Gov. Rick Scott signed a law barring Florida doctors from routinely asking patients if they own a gun. The law also authorizes patients to report doctors for “unnecessarily harassing” them about gun ownership and makes it illegal to routinely document firearm ownership information in a patient’s medical record. Other state legislatures have considered similar proposals, but Florida is the first to enact such a law…
The measure was introduced in the state Legislature after a pediatrician in Central Florida dismissed a mother from his practice when she angrily refused to answer a routine question about whether she kept a gun in her house. The doctor, Chris Okonkwo, said at the time that he asked so he could offer appropriate safety advice, just as he customarily asks parents if they have a swimming pool and teenagers if they use their cellphones when they drive. He said that he dismissed the mother because he felt they could not establish a trusting doctor-patient relationship.
Aaron Carroll, a pediatrician, explains why he’s asking these questions.
I ask parents regularly if they have a gun in the home. If they tell me they do, I ask how it’s stored. I recommend that they think about not having a gun around children. If they must, I recommend that they keep it unloaded, locked up, with the bullets stored separately.
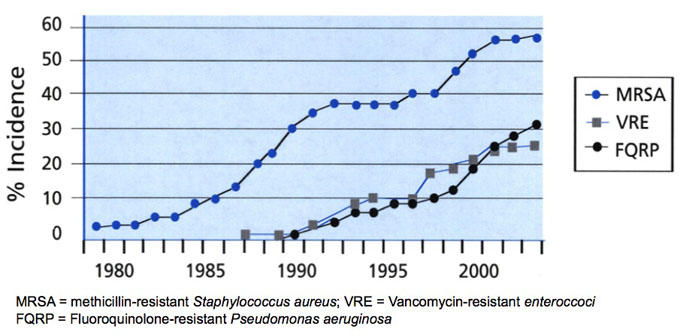
Why? Because in 2005, guns were were in involved in almost 85% of homicides and more than 45% of suicides in children aged 5-19 years, not to mention many accidents. I ask about guns because they are a major mechanism of childhood death. I’m trying to prevent that from happening.
I’m not judging my patients or harassing them, any more than when I ask them whether they use bike helmets, or whether they use car seats, or whether they let their kids cross the street unaccompanied by an adult. I’m trying to keep them from getting killed. That’s my job.
Dr. Carroll says that it’s his job to keep my children from being killed. That it’s his job to ask questions about how I instruct my children and what precautions I take. That it’s his job to oversee the general safety and security of my home and possessions.
I think that, in effect, makes him my parent. It puts me in a position of being answerable to him, of needing his approval of how I live and act. It takes away the responsibility that I have, for my children. He’s making them his responsibility.
This reminds me of the “Oath of Responsibility” that Residents of Grainne take, in the book Freehold.
I,, before witness, declare myself an adult, responsible for my actions, and able to enter contract. I accept my debts and duties as a Resident of the Freehold of Grainne.
It’s a simple oath, but a very deep one. Simply, it declares that I’m responsible for my own actions. Deeply, it means that I agree to accept any and all consequences for my actions—good or bad. There’s no one I can blame if things go disastrously wrong. There’s no one backstopping me if I start to veer into a ditch. There’s no one hovering over me, waiting to snatch me back from the brink of disaster.
It’s a sobering oath. If I take it seriously, it would mean that I have to slow down and carefully think through all of the potential consequences for the decisions I make. It means that I need to be sure, quite sure, before I act.
This is what being responsible looks like. This is what it means to be an adult. And this is the oath that I implicitly took when I moved away from home and, especially, when I got married. I did both of those things years before I read Freehold and read this oath. But this oath resonated with me, the first time I read it. It explicitly stated what I’d always implicitly assumed and lived by.
That’s why I resent these pediatricians who think it’s their job to look out for my children and who think that it’s their job to question and second guess my decisions. I took responsibility for my children long before I had them. I retain responsibility for them now. And I am not going to outsource that responsibility to anyone, no matter how well intentioned they may be.
No, Dr. Carroll, keeping my children safe and alive isn’t your job. It’s mine. You are not responsible to monitor whether (or when) my children wear bike helmets, when they stop using car seats, or when I let them cross the street unaccompanied by an adult. It’s my responsibility.
I have a dual responsibility: to protect them from harm and to teach them how to live responsibly. I have a responsibility to teach them how to distinguish something that’s truly dangerous (riding a motercycle on the highway without a helmet) from something that’s merely occasionally a little risky (riding a toddler bike on the sidewalk without a helmet).
I have a responsibility to teach them how to safely cross the street. Eventually, that will result in me letting them walk to the park unaccompanied by an adult. In doing so, they’ll cross one or two streets, unaccompanied by an adult. I have to teach them how to do that. Invevitably, they’ll end up doing it sooner than I think, at a time when I’m not prepared for them to do so. When that happens, I want them to already know how to do it safely—not to be completely unprepared because their pediatrician thought it was reckless and dangerous.
Dr. Carroll, if I ever come into your office, it’s because I want you to do the job I cannot do: the job of knowing which medicines and treatments will heal my kids after they get hurt or after they get sick. If you can do that, we can have a good, strong, relationship. If you try to take responsibility for my household and try to take authority that I haven’t given you, we’re going to have problems.